The University of the Free State (UFS)
Department of Nuclear Medicine has, for the first time, started using Lutetium 177 PSMA (Lu-177 PSMA) therapy for the treatment of metastatic castrate-resistant
prostate cancer (MCRPC) – an advanced stage of prostate cancer.
The UFS and the Free State province are now joining other South African universities, such as the University of Pretoria, the University of the Witwatersrand, and other provinces in using this method to treat MCRPC patients.
Dr Osayande Evbuomwan, a Senior Lecturer and medical specialist in the Department of Nuclear Medicine,
Faculty of Health Sciences, says they have started treating their first MCRP patient (first cycle) with peptide receptor
radionuclide therapy (PRRT) on 15 July. It is the first time that Lutetium 177 PSMA – a type of PRRT used for treating patients with MCRPC – has been used in the Free State. This method is used on MCRPC patients who are not eligible for
chemotherapy or have failed first- or second-line chemotherapy.
Expertise and funds are now available for this treatment
Dr Evbuomwan was trained and exposed to this therapy at the University of the Witwatersrand during his registrar training in nuclear medicine. When he joined the UFS in 2019, he – with the always available help of the Head of Department, Dr Gerrit
Engelbrecht – pushed for the therapy to be used in the department.
“We in the Department of Nuclear Medicine are happy that expertise is now available and that some funds have been released for this treatment to commence. The index patient is very sick with MCRPC and was too sick to qualify for first-line chemotherapy.
Each patient will need about four-six cycles for complete treatment. The patient is being treated in the Department of Nuclear Medicine at the Universitas Academic Hospital and Annex.”
“We are hoping that he will be able to complete at least four cycles and respond well to the treatment. We believe that the ability to administer this treatment now is good news for the Free State, as the people of the Free State also deserve to
be exposed to this level of treatment. We are hoping that the government will continue to provide more funds for more of these patients to be treated in our facility,” says Dr Evbuomwan.
It was budgeted to treat five patients (20 cycles), with each cycle (just the Lu-177 PSMA) costing more than R50 000.
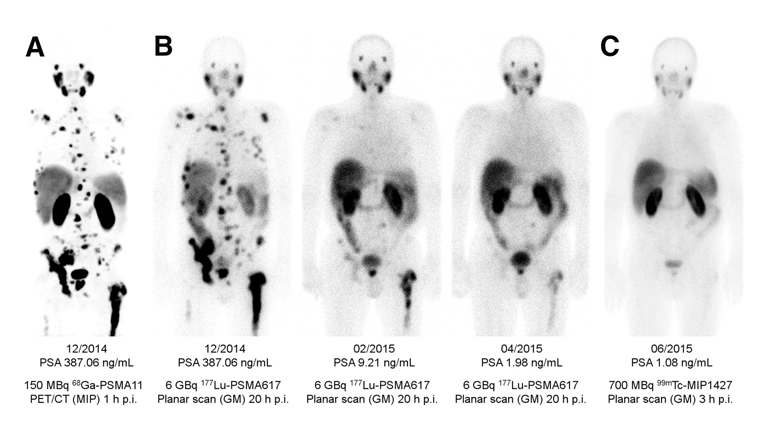
A googled image from the internet of a case before, during, and after completing the full course of therapy. The first image is before
treatment and the last image is after completing treatment, while the images in between are during treatment. (Source: Google)
Prostate cancer one of the leading causes of morbidity and mortality
Dr Evbuomwan says prostate cancer is one of the leading causes of morbidity and mortality in the world, including South Africa. When it progresses to the advanced stage of MCRPC, the prognosis becomes bad.
Dr Evbuomwan explains that there are various conventional systemic therapies, including first- and second-line chemotherapy that could be used to treat patients at this bad stage. However, not all patients are fit for chemotherapy. The few who are
fit, according to Dr Evbuomwan, usually end up failing the first-line chemotherapy, which has a lot of undesirable side effects and require long-stay hospital admissions.
Only a few centres are able to offer second-line chemotherapy. So many of these patients end up suffering from prolonged bone pains before eventually dying from the disease.
PRRT is a targeted nuclear medicine therapy that offers the opportunity to deliver very high levels of radiation specifically to cancer cells, because these cancer cells express specific receptors to which certain peptides can bind. This specificity to
cancer cells offers the advantage of providing lower doses of radiation and damage to normal organs and tissues, a characteristic that conventional therapies do not offer, explains Dr Evbuomwan.
According to him, Lutetium 177 PSMA (Lu-177 PSMA) is a type of PRRT used for treating patients with MCRPC, who are not eligible for chemotherapy or have failed first-line chemotherapy. Numerous research studies around the world have proven that this treatment
improves quality of life, slows down disease progression, and improves overall survival, with little or very tolerable side effects in most patients.
The University of Pretoria is one of the pioneers of this treatment in the world, having done a lot of research with it since 2017. Other provinces such as the Western Cape and KwaZulu-Natal have also recently become involved with the therapy. This therapy
is expensive and requires a lot of expertise. It also involves the input of a multidisciplinary team (MDT), which must at least include a nuclear medicine physician, a radiation oncologist, and a urologist. The Departments of Urology and Radiation
Oncology at the UFS were also instrumental in the initiation of the therapy and form part of the MDT team at the UFS in the management of these patients.
Treatment puts department, university, and hospital on the map
Dr Evbuomwan says the ability to administer this treatment puts the department, the UFS, and the hospital on the map, alongside other top universities within and outside the country. “It also creates an avenue for us to gather data for research
purposes and for publications. We are now able to offer a promising, safe, and highly efficacious therapy for patients with MCRPC in the Free State. Some of these patients no longer need to travel to other provinces to get the treatment.”
There are plans to expand the treatment to more patients – and hospital management, who were present at the first treatment, are excited and looking forward to the outcome of this current treatment.
Watch video below: