 |
|
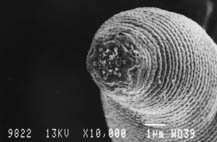
Halicephalobus mephisto (Devil’s Worm)
Photo: Supplied
29 May 2012
|
A minuscule little worm found and researched with the assistance of researchers at the university has made it onto the list of Top 10 New Species of the world. The list was published by the International Institute for Species Exploration (IISE) at Arizona State University and a committee of scientists from around the world. It lists the top ten new species described in 2011.
An article on the new worm species appeared in the authoritative journal Nature in June 2011.
Prof. Esta van Heerden, leader of the university’s research team, says, “In our wildest dreams, we could not have imagined that we would get so much reaction from the worm’s discovery. We had to do so many checks and balances to convince Nature that the worm could survive in the old and warm water. We were very excited when the article was accepted but the media reaction was unbelievable.”
The tiny nematode, Halicephalobus mephisto (Devil’s Worm) of about 0,5 mm in length, is the deepest-living terrestrial multi-cellular organism on earth. It was discovered in the Beatrix gold mine near Welkom at a depth of 1,3 km.
The IISE says in a statement the species is remarkable for surviving immense underground pressure as well as high temperatures. The borehole water where this species lives has not been in contact with the earth’s atmosphere for the last 4 000 to 6 000 years.
This top-10 list includes a sneezing monkey; a beautiful, but venomous jellyfish; a fungus named after a popular TV cartoon character; a night-blooming orchid; an ancient walking cactus creature; and a tiny wasp. A vibrant poppy, a giant millipede and a blue tarantula also made it onto the list.
The international selection committee made its choice from more than 200 nominations. They looked for species that captured the attention because they were unusual or because they had bizarre traits. Some of the new species have interesting names.
Prof. Van Heerden says, “We are very thankful for the exposure that the university gets as a result of the inclusion on the list and we enjoy the international cooperation immensely.”